• Lab data often play crucial role in guiding diagnosis and management in patients with suspected sepsis.
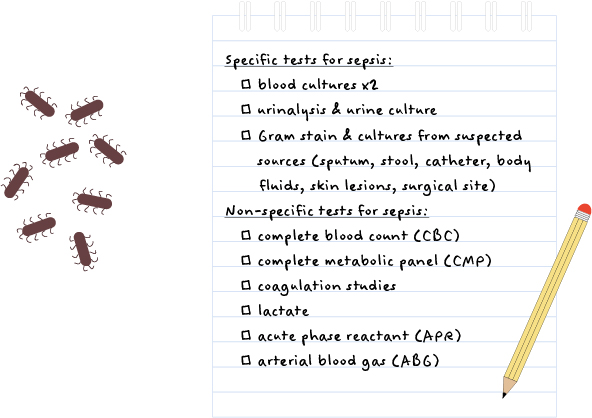
• Tests used to identify source of infection include:
Blood cultures (either peripherally via venopuncture or centrally via central line sampling): to evaluate for bacteremia and associated risk of endocarditis and systemic spread and to guide antibiotic treatment (IV vs PO)
Urinalysis and urine culture: if suspected urinary tract infection
Additional microbiological studies of samples can be obtained, if suspicion is high, from other body sites including sputum, stool, catheter/line, body fluids (peritoneal, pleural, CSF), skin lesions, surgical wound
• Tests used to assess for the severity of illness and extent of organ damage (and response to treatment) include:
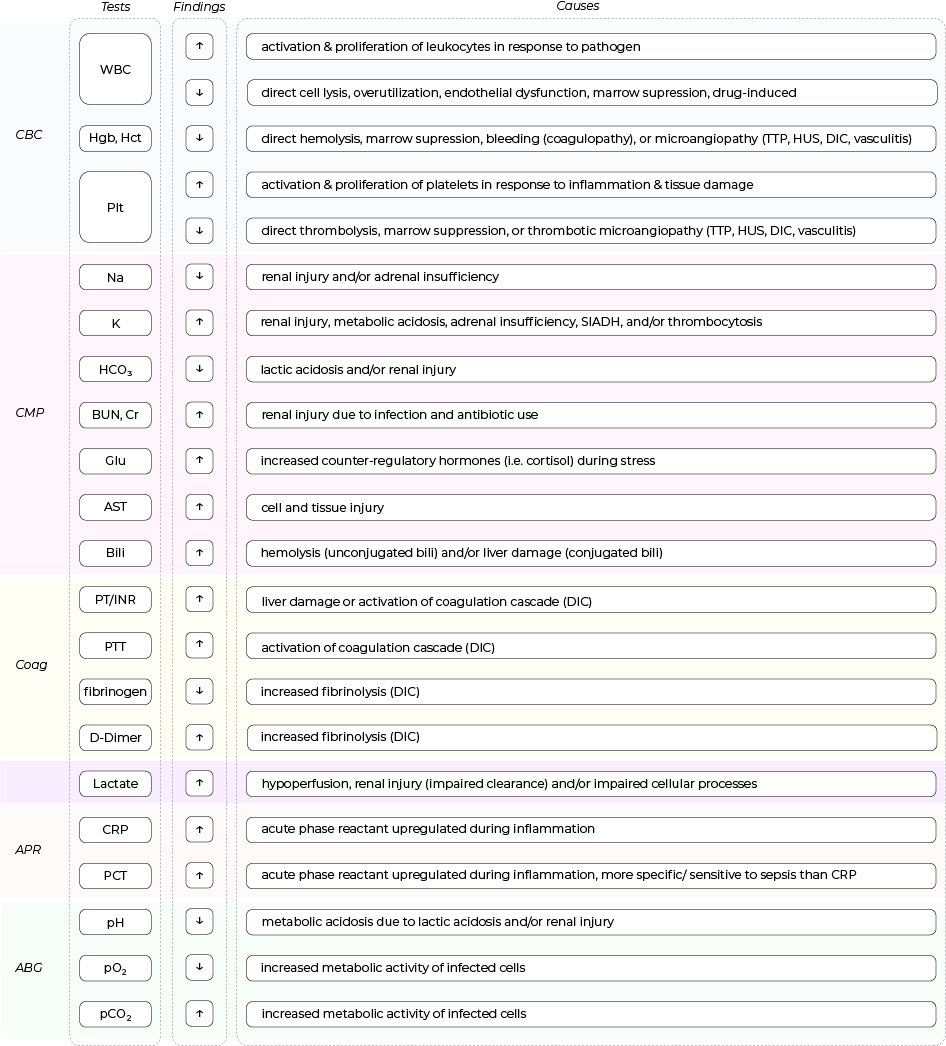
CBC with differentials: acute infection might cause reactive leukocytosis and thrombocytosis (in contrast, leukopenia and thrombocytopenia are signs of severe sepsis), with or without anemia depending on the culprit microorganisms
Coagulation studies: might be abnormal, especially in the case of disseminated intravascular coagulopathy (DIC)
CMP: electrolyte disturbances, renal, and/or liver dysfunction might be seen
Inflammatory markers including C-reactive protein (CRP) and procalcitonin (PCT) might be elevated
Lactate: might be elevated depending on the severity of sepsis causing hypoperfusion and impaired cellular metabolism
ABG: might show acidemia, hypoxemia (+/- hypoxia), and hypercapnia
• The mechanisms behind abnormal lab findings commonly seen in septic patients are listed in the table below.