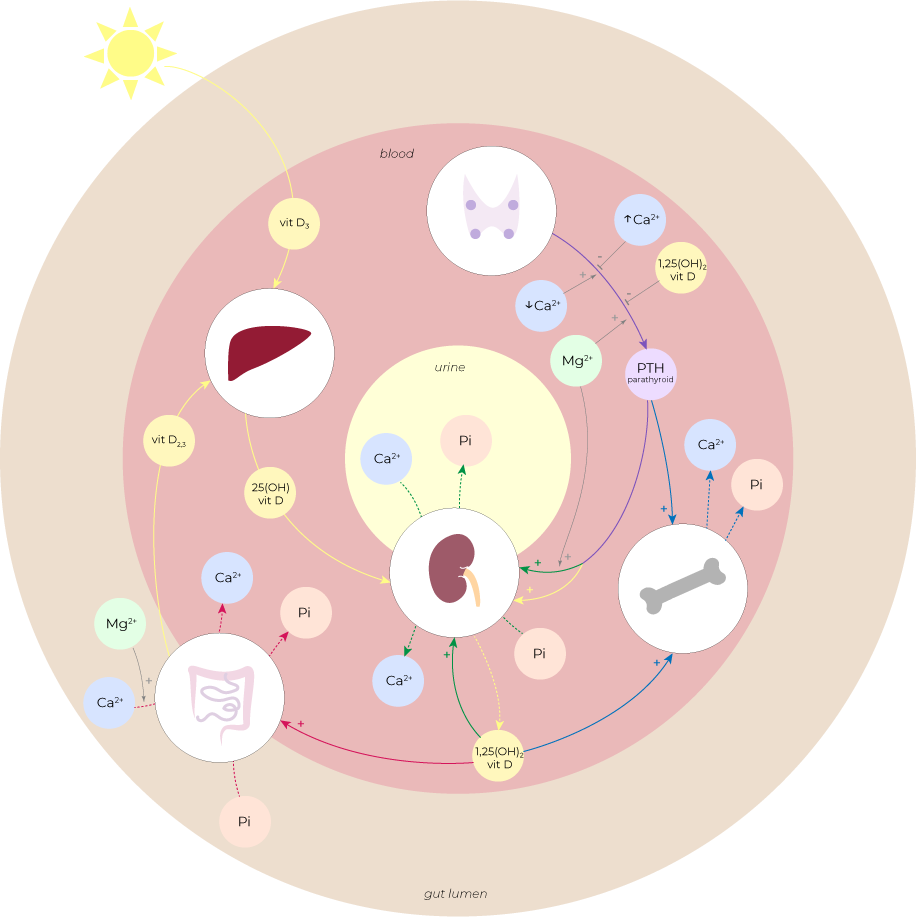
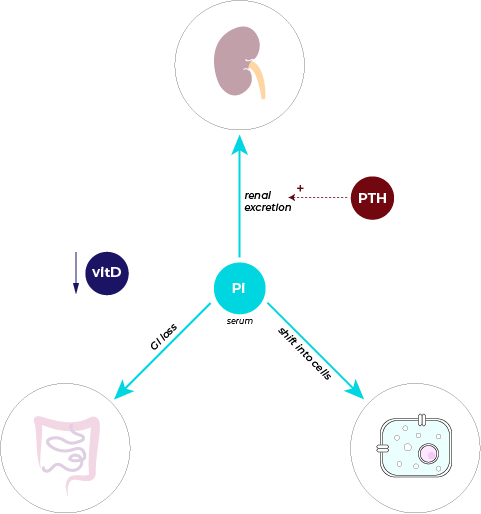
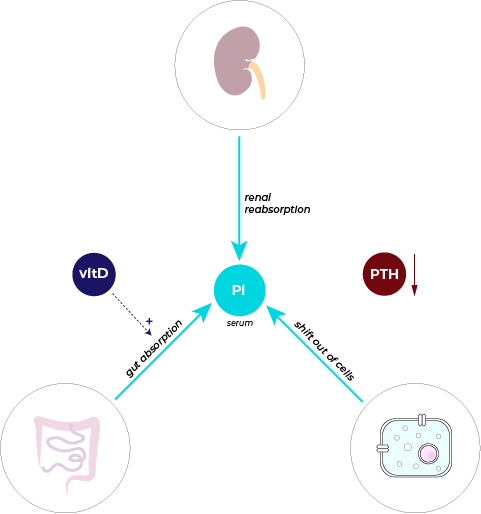
• Inorganic phosphorous (Pi) compounds (mainly in the forms of PO43-, HPO42-, H2PO4-) move between the blood vessels and 4 different body compartments:
Renal tubule: via renal reabsorption and excretion mechanisms
Bone: via bone deposition and resorption
Gut lumen: via absorption and secretion across GI cells
Intracellular space: via movement across ion channels
• Pi imbalance arise when their movements between these body compartments are disregulated.
• Some of the regulators of Pi are parathyroid hormone (PTH) and vitamin D:
PTH: via renal reabsorption and excretion mechanisms
Vitamin D: via absorption and secretion across GI cells