

• Hypernatremia is defined as serum sodium concentration above 145 mEq/L.
• Hypernatremia is caused by either decreased water or increased salt concentration in the blood which is driven by the kidneys' handling of sodium and water.
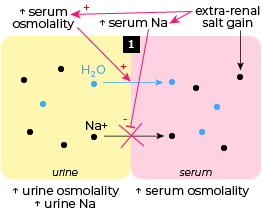
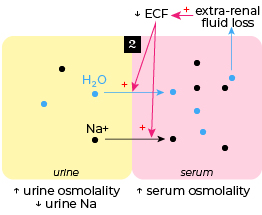
• The causes of hypernatremia can be determined based on urine osmolalilty and urine sodium level.
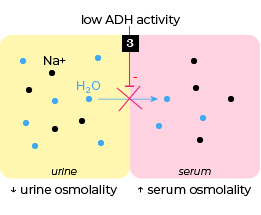
Urine osmolalilty: reflects renal water handling (via aquaporins-V2 receptors), decreases when water is excreted and increases when water is reabsorbed, often influenced by the level of ADH activity.
Urine sodium: reflects renal sodium handling (via Na channels), decreases when Na is reabsorbed and increases when Na is excreted.
• One diagnostic approach for hypernatremia is illustrated below.
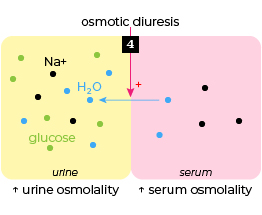
Urine osmolality is low (< 300 mOsm/kg or < serum osmolality) in diabetes insipidus and intermediate (300-600 mOsm/kg and > serum osmolality) in osmotic diuresis.
If urine osmolality is high (> 600 mOsm/kg), urine sodium concentration (uNa) is used to further differentiate between extra-renal salt gain causes (uNa > 40 mmol/L), and extra-renal net water loss causes (uNa < 25 mmol/L).







