no

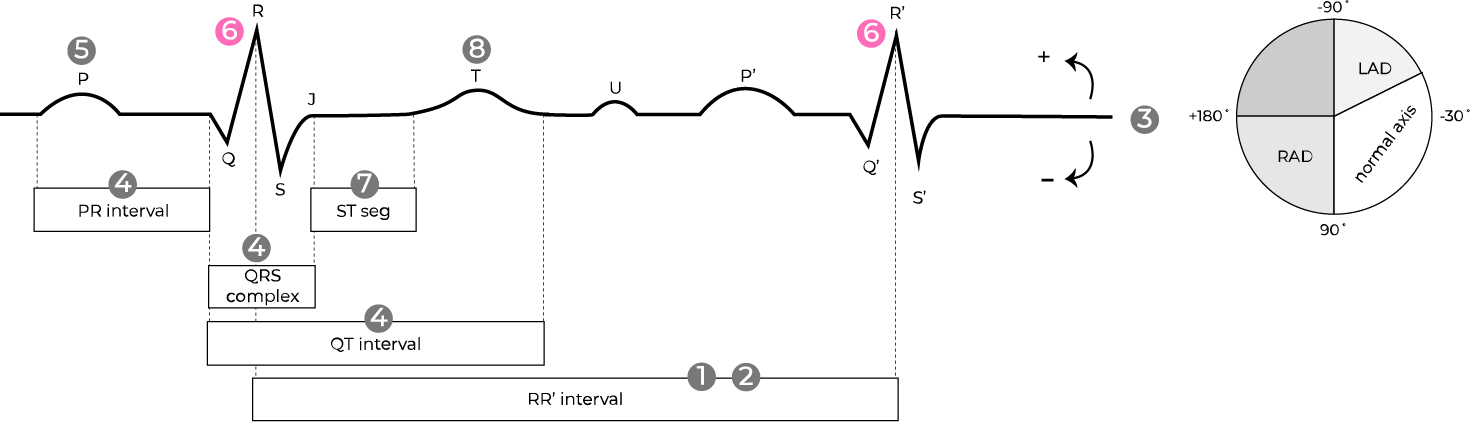
small, narrow q wave
(normal septal depolarization, often in left-sided leads, I, avL, V5-6)

myocardial cells in the ventricular septum depolarize and also pull net electrical vectors away from lateral leads avL and V6 resulting in the first portion (small q) of QRS complex to be negatively deflected