





• In acute pericarditis, there is a generalized inflammation of the pericardium thus affecting both the ventricles (ST-T changes) and atria (PR changes).
• As a result, ECG changes are seen in most, if not all, leads including:
ST elevation--
diffuse, in both anterior and inferior precordial leads, with reciprocal ST depression in aVR
upward concavity morphology
less prominent than in STEMI
PR depression--
diffuse, in both anterior and inferior precordial leads, with reciprocal PR elevation in aVR (”knuckle sign”)
is discordance with ST segment (i.e. PR depression & ST elevation in the same lead)
T inversion--
only seen on occasions
less prominent than in STEMI
• Comparing to STEMI, ST-T changes in acute pericarditis are diffuse, and there is no Q wave nor reciprocal ST depression.
• Comparing to benign early repolarization, ST elevations in acute pericarditis don’t persist over time.



• In pericardial effusion, the accumulated fluid surrounding the heart acts as an insulator causing a reduce in electrical signals detected by the ECG electrodes.
• This results in low voltage of QRS complexes on ECG.

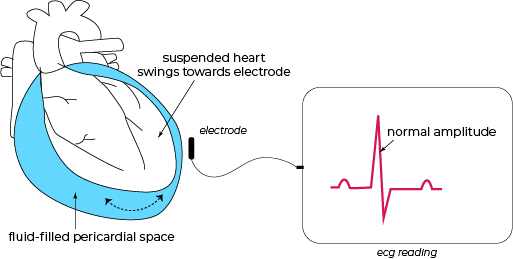
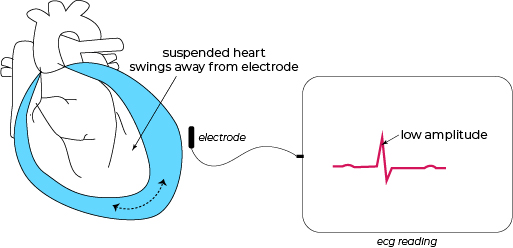
• In massive pericardial effusion or cardiac tamponade, the heart is suspended and swings back and forth in the perdicardial sac filled with a massive amount of fluid.
As the heart swings towards the chest where the ECG electrodes are placed, the recorded rhythm has a normal amplitude
As the heart swings away from the chest where the ECG electrodes are placed, the recorded rhythm has a lower amplitude
• This results in electrical alternans which is beat-to-beat shift in QRS axis, in addition to low voltage and sinus tachycardia.






